 日本語
日本語  Deutsch
Deutsch  English
English  Español
Español  Français
Français  Português
Português 
There are very few conversations in men's health that generate more noise and less signal than the one about size. Forums, locker rooms, adult entertainment, and the comment sections of dubious "enhancement" websites have been polluting the data pool for decades.
Into all of that noise, a 2015 paper published in the British Journal of Urology International (BJUI) dropped something rare: actual, clinically measured, peer-reviewed numbers collected from more than 15,000 men.
That study — a systematic review and meta-analysis led by Dr. David Veale and a team of researchers — did not set out to make anyone feel better or worse about themselves. It set out to establish medical baselines. The findings have since become a reference point for urologists, psychologists treating body dysmorphic disorder, and condom manufacturers calibrating sizing standards. The data is worth understanding — not because it tells you who you are, but because most of what you've heard before this probably wasn't true.
At a Glance · Meta-Analysis · N = 15,521 Men
The Bottom Line
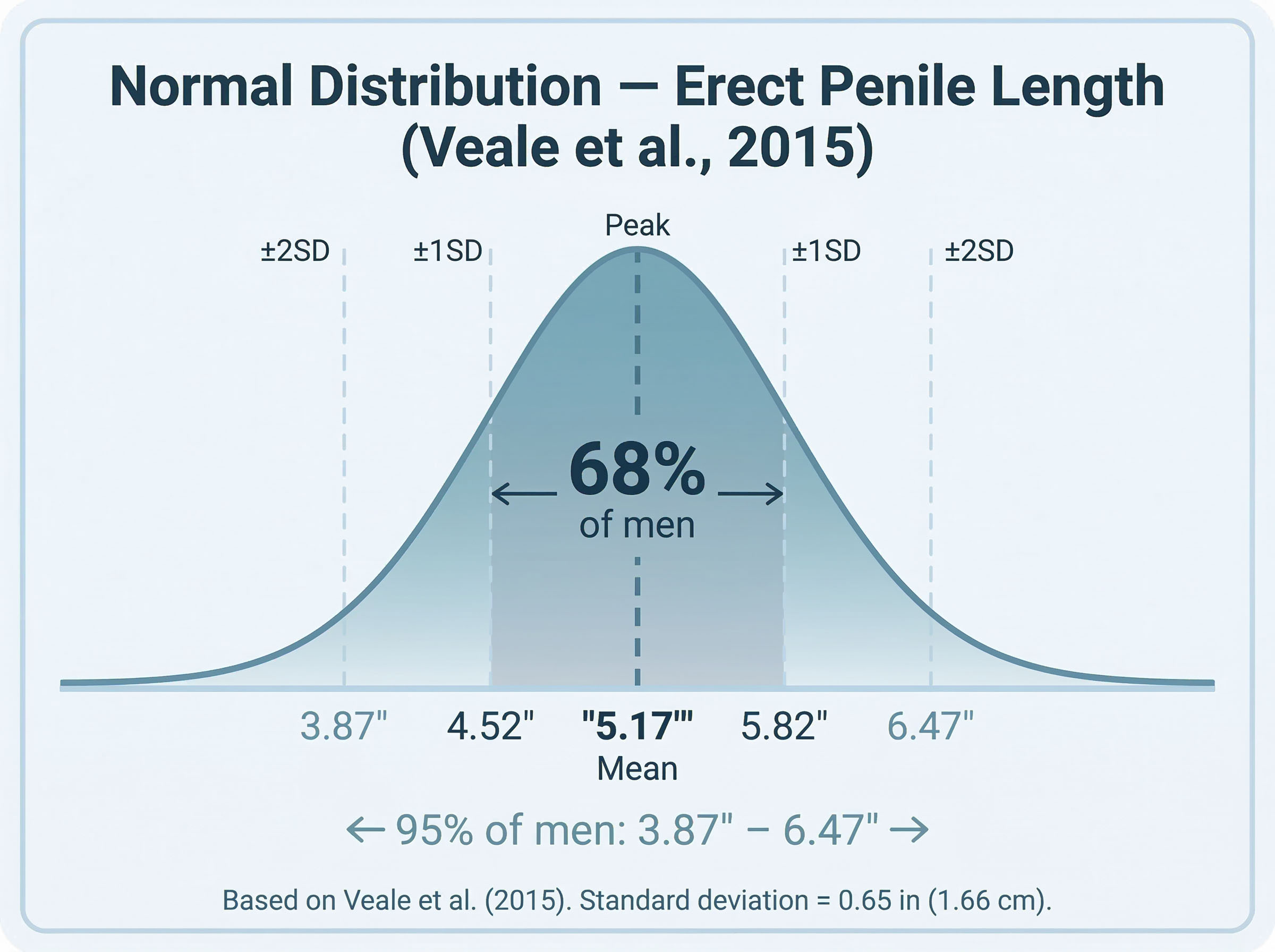
The largest clinician-measured study on record puts the mean erect penile length at 5.17 inches (13.12 cm), with a standard deviation of roughly 0.65 inches (1.66 cm). Anything between about 4.5 and 5.8 inches sits squarely in the middle of the normal distribution — a zone that covers the majority of men on earth.
Source: Veale et al., British Journal of Urology International, 2015
"The study didn't set out to make anyone feel better or worse. It set out to establish medical baselines — and that is exactly what it did."
— Adrian Lowe
Why This Study Stands Above the Rest
Before 2015, most of the data floating around about penile dimensions came from self-reported surveys. Men were given a ruler, asked to measure themselves, and trusted to report their findings honestly. That methodology has an obvious problem: it skews high. Research on self-reported health data consistently finds that men overestimate height, weight lifted, income, and — as multiple analyses have confirmed — penile length by a meaningful margin.
The Veale et al. meta-analysis cut through that bias by restricting its data pool almost entirely to clinician-measured studies. A researcher, not the subject, held the measuring instrument. The study aggregated data from 20 studies involving 15,521 men across multiple countries. Every measurement followed a standardized protocol: erect length was measured from the pubic bone to the tip of the glans (called the bone-pressed erect length, or BPEL), and flaccid measurements were similarly standardized.
This is why the paper remains the most-cited piece in the field. It isn't perfect — no single study is — but its methodology is rigorous by any clinical standard.
Methodology Note
Bone-Pressed Erect Length (BPEL): Measured from the pubic symphysis (the bone at the base of the penis) to the tip of the glans while erect. This is the clinical gold standard because it removes variation caused by pubic fat pad thickness — meaning two men with the same underlying penile structure measure equally, regardless of body composition. Non-bone-pressed measurements are what most men take at home, which can read 0.5–1 inch shorter in men carrying extra weight around the abdomen.
The Core Numbers: Breaking Down the Data
Here is what the study actually found, presented without agenda:
Table 1 — Summary Measurements from Veale et al. (2015), N = 15,521
Understanding the Bell Curve: Normal Is Not a Single Number
The mean is one number. The distribution is the full story. Understanding the standard deviation changes the way most men should think about where they fall on the scale.
With a mean of 5.17 inches and a standard deviation of 0.65 inches, basic statistics tells us the following:
- 68% of men fall between 4.52 and 5.82 inches.
- 95% of men fall between 3.87 and 6.47 inches.
- 99.7% of men fall between 3.22 and 7.12 inches.
Read that again. A man measuring 6.3 inches erect is in roughly the top 5% of the population — but by the numbers, he is still within two standard deviations of the mean. That is not an outlier. That is a well-distributed tail of a normal curve. Similarly, a man at 4.7 inches sits below the mean — but still within the central 68% of all men measured in the largest study ever conducted on this subject.
Did You Know?
Flaccid length is a notoriously poor predictor of erect length. Men classified as "growers" can increase by 50–100% or more during erection, while "showers" — men with larger flaccid dimensions — may increase proportionally less. Neither type has a measurable advantage in erect size over the other.
Growers vs. Showers — And Why Flaccid Comparisons Mean Nothing
The anxiety most men experience isn't grounded in erect measurement at all. It's rooted in locker room comparison — a context in which every man is flaccid and none is a reliable benchmark for anything. This is where the grower-versus-shower distinction becomes medically significant.
Research published in the Journal of Sex and Marital Therapy found that roughly 79% of men are "growers" — meaning their flaccid length increases by more than 50% upon erection. The remaining 21% are "showers" who present larger flaccid but experience a proportionally smaller increase when aroused. The takeaway is straightforward: flaccid appearance is not predictive of erect size in any consistent way. Comparing flaccid dimensions is comparing apples to engine parts.
What the Study Does Not Claim — Correlation, Causation, and the Myths That Won't Die
The Veale et al. study was careful about what it measured and what it didn't. It did not make causal claims about what predicts size. That hasn't stopped decades of pop-science from trying. Here are the most persistent myths, measured against what the data actually shows:
Table 2 — Common Predictors: What the Research Actually Shows
Cultural Insight
The Measurement Problem Across Cultures
Studies contributing to meta-analyses like Veale et al. were conducted across different countries, including the UK, Germany, Brazil, South Korea, and the US. Different laboratory settings, recruitment methods, and cultural attitudes toward participation all introduce variability. This is why the study's methodology note — clinician-measured only — was so important. It removed the largest single variable: the man's own desire to impress a researcher with a measuring tape.
The Psychological Weight Nobody Talks About Honestly
The Veale et al. study wasn't commissioned purely for anatomical curiosity. Its most direct clinical application was in the treatment of penile dysmorphic disorder (PDD) — a condition in which a man becomes preoccupied with the belief that his penis is abnormally small, even when clinical measurement places him within the normal range or even above average.
That condition is more prevalent than most people realize, and it shares diagnostic overlap with body dysmorphic disorder (BDD) — a well-documented psychological condition classified in the DSM-5. Research led by Dr. Veale himself, published in separate papers, found that men with PDD consistently underestimate their own size relative to the established mean, regardless of their actual measurements.
This is the place where hard data intersects with mental health — not to provide a substitute for professional care, but to establish a fact-based floor: most men who believe they are abnormally small are, according to clinician measurement, not. That is not a platitude. That is what the data shows.
"Men with penile dysmorphic disorder consistently underestimate their own size relative to the mean — regardless of their actual measurements. That is not a psychological quirk; that is a documented clinical pattern."
The Pornography Variable: Why the Reference Frame is Broken
Any honest analysis of why men misjudge their own size has to confront the most obvious distortion in the room. The adult entertainment industry selects performers based on physical characteristics that sit, by definition, at the extreme right tail of any normal distribution. Presenting that repeatedly as a normative frame of reference is the statistical equivalent of watching elite NBA players and concluding that everyone who can't dunk has below-average height.
This isn't a moral argument. It's a mathematical one. If the mean erect length across 15,000 clinician-measured men is 5.17 inches, and the median performer in certain content categories measures measurably above 7 inches, the viewer is not seeing average. He is seeing a statistical outlier — selected for exactly that characteristic — and comparing himself to it.
Research published in the Journal of Sex Research has connected heavy consumption of explicit content with distorted body image in men, including inflated estimates of what constitutes "normal" size. The data from Veale et al. is a corrective to that distortion — a documented, peer-reviewed baseline that most men will find more favorable to their actual position than the frame of reference they've been working with.
In Brief
- The Veale et al. (2015) meta-analysis studied 15,521 men using clinician-measured data — the gold standard in this research field.
- Mean erect length (bone-pressed): 5.17 inches / 13.12 cm
- Mean erect girth: 4.59 inches / 11.66 cm
- Standard deviation of ±0.65 inches means 68% of men fall between 4.52 and 5.82 inches.
- No strong correlation exists between penile size and height, shoe size, or hand size.
- Flaccid length is not a reliable predictor of erect length.
- BMI affects visible length but does not change actual bone-pressed erect length.
- The study was designed in part to establish clinical baselines for treating penile dysmorphic disorder.
What the Study Didn't Cover — And Why That Matters
The Veale et al. paper is comprehensive in its scope, but it has acknowledged limitations that are worth stating plainly:
Geographic and ethnic representation: The 20 contributing studies were drawn largely from populations in Europe, North America, and parts of Asia. The authors noted that sample composition varied, and that drawing cross-regional or cross-ethnic conclusions was not supported by their methodology. Anyone claiming this study proves anything about size differences between ethnic groups is misreading it.
Age distribution: The studies aggregated did not uniformly report participant age ranges. Penile dimensions can be affected by hormonal changes associated with aging, so a younger-skewed sample might not perfectly represent all adult males.
Erection quality as a variable: The study measured clinician-induced erections, typically achieved through pharmacological means (injection of a vasoactive agent). This standardizes measurement but may not perfectly replicate naturally occurring erections, which can vary based on arousal level, stress, and vascular health.
These limitations don't undermine the study's core findings — they just define its scope. And within that scope, it remains the most reliable data set available on this subject.
Q&A: What Men Actually Want to Know
The Takeaway from 15,000 Men
The 2015 British Journal of Urology International study is worth reading not because it settles every question, but because it replaces noise with data. The mean erect length of 5.17 inches, with a standard deviation of 0.65 inches, means that the normal range is wide — far wider than most men believe based on the reference points available to them in popular culture.
The study's authors were primarily motivated by clinical utility. They wanted a reliable baseline for surgeons evaluating corrective procedures, for psychologists treating body-image disorders, and for researchers designing any future work in this area. What they produced incidentally is the best available evidence against a particular kind of anxiety that affects men in silence — an anxiety that, according to the data, is frequently built on a distorted sense of where they actually stand.
The numbers don't lie. Most men are normal. Most men have been measuring themselves against a warped ruler. And now, at least, the corrected scale exists — peer-reviewed, clinician-measured, and published for anyone willing to check.
Sources & Further Reading
- Veale D, Miles S, Bramley S, Muir G, Hodsoll J. (2015). Am I normal? A systematic review and construction of nomograms for flaccid and erect penis length and circumference in up to 15,521 men. BJU International, 115(6), 978–986.
- Shaeer O, Shaeer K. (2012). The Global Online Sexuality Survey. Journal of Sexual Medicine.
- Promodu K et al. (2007). Penile length and circumference: an Indian study. International Journal of Impotence Research.
- Herbenick D et al. (2014). Erect penile length and circumference dimensions of 1,661 sexually active men in the United States. Journal of Sexual Medicine.
This article analyzes published clinical research and does not constitute medical advice. Consult a qualified healthcare provider for personal health concerns.
Disclaimer: The articles and information provided by Genital Size are for informational and educational purposes only. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition.

